GLP-1 medications have been racking up an unusually long list of benefits beyond their original purpose. First approved for type 2 diabetes, then established as genuinely effective weight loss drugs, they’ve since been linked to fewer heart attacks and strokes, improved sleep apnea, slower kidney disease progression, and reduced fatty liver disease. In June 2026, breast cancer was added to that list — and the size of the effect reported was large enough to catch the attention of oncologists who don’t typically get excited about observational data.
Here’s what the new research actually found, how strong the evidence really is, and why even the researchers behind these studies are being careful not to oversell it.
What the New Studies Actually Found
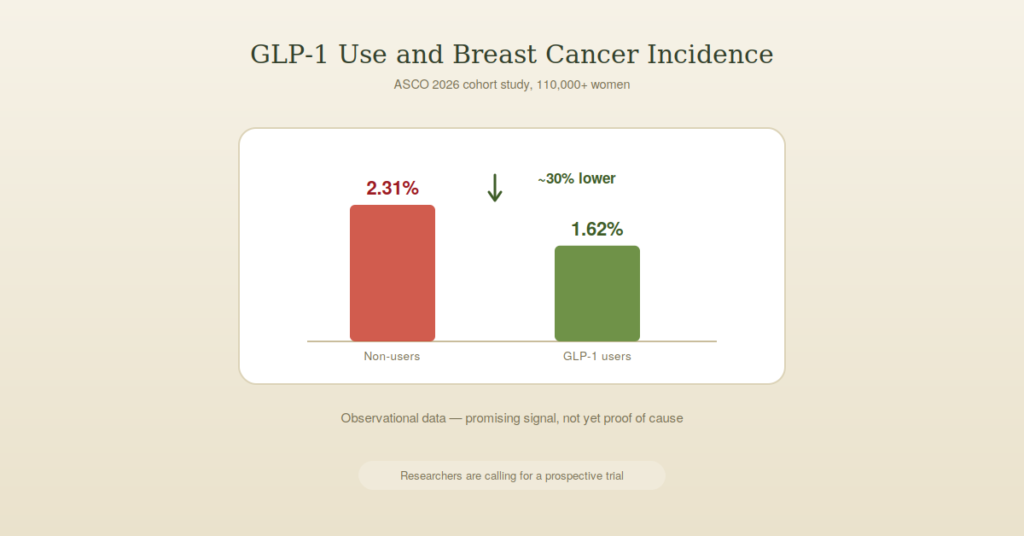
The headline finding came from a large retrospective study presented at the 2026 American Society of Clinical Oncology Annual Meeting in Chicago in early June, led by Dr. Elizabeth McDonald, a breast radiologist and professor of radiology at the University of Pennsylvania’s Perelman School of Medicine. The study examined more than 110,000 women between the ages of 45 and 80 who underwent breast imaging, comparing breast cancer rates between those who had taken GLP-1 medications and those who hadn’t.
The results were striking. In the matched analysis, breast cancer occurred in 1.62% of GLP-1 users compared with 2.31% of non-users — a roughly 30% relative reduction in risk. A separate, smaller study presented at the same meeting, following more than 80,000 women specifically considered high-risk for breast cancer, found a somewhat more modest but still meaningful 16% reduction. Reporting on the broader body of emerging research described findings across different studies ranging from 30% to as high as 47% risk reduction, depending on the specific population studied and how the analysis was structured.
One detail researchers highlighted as reassuring: the reduction held up when Black and White women were analyzed separately, suggesting the effect wasn’t isolated to one demographic group within the study population.
Why Researchers Don’t Think This Is Just About Weight Loss
The obvious first explanation is that GLP-1 drugs cause significant weight loss, and excess body fat is already a well-established risk factor for breast cancer, particularly after menopause. That’s clearly part of the story. But several of the researchers involved have pointed to mechanisms beyond simple weight reduction.
Dr. Neil Iyengar, a breast medical oncologist who was not involved in either study, told Medscape Medical News that the more weight loss a patient experiences, the greater the reduction in breast cancer risk appears to be — supporting weight loss as a major contributor. At the same time, he noted that GLP-1 receptor agonists have broader effects across multiple biological pathways connecting obesity to cancer, including pathways related to insulin resistance and chronic inflammation, not just the simple fact of reduced body fat.
This lines up with the biological mechanisms researchers have proposed: GLP-1 drugs reduce hyperinsulinemia, or chronically elevated insulin levels, and improve insulin sensitivity, which in turn lowers signaling through a growth pathway called IGF-1 that’s been linked to cancer cell proliferation in laboratory research. They also appear to reduce inflammation in fat tissue itself, which matters because adipose tissue inflammation is increasingly understood as a contributor to cancer risk, separate from body weight alone.
Interestingly, a researcher named Dr. Jennifer Ligibel pointed to preclinical research in mice that adds an important nuance: in those animal studies, a very-low-calorie diet actually shrank tumors more than a GLP-1 receptor agonist did, suggesting weight loss itself, however it’s achieved, may be doing a substantial share of the work — with the medication potentially adding something on top of that, rather than working through a completely separate mechanism.
The Important Caveats Researchers Are Emphasizing
This is the part of the story that’s easy to skip past in an exciting headline, and it’s worth taking seriously, because the researchers themselves are being unusually direct about it.
Dr. McDonald, the lead author of the largest study, stated plainly to the ASCO audience that observational studies are “hypothesis generating” and that they “do not demonstrate causality.” This is a meaningful scientific distinction. The study can show that women who happened to take GLP-1 medications developed breast cancer less often than women who didn’t — but it cannot prove the medication itself caused that difference, rather than some other factor that happened to be more common among GLP-1 users, such as more frequent medical checkups, different baseline health status, or other unmeasured lifestyle differences between the two groups.
The American College of Radiology, which managed one of the studies, was explicit in calling for a large prospective study, a more rigorous design that would track patients forward in time after deliberately assigning or observing GLP-1 use, specifically to clarify whether the drugs actually cause reduced cancer incidence or simply correlate with it.
Read more What Is GLP-1 and Why Do Doctors Say It Is the Key to Weight Loss
There’s also the matter of absolute versus relative risk, which is worth understanding clearly. A 30% relative risk reduction sounds dramatic, but the actual absolute difference in this study was 0.69 percentage points — roughly seven fewer breast cancer cases per 1,000 women studied. Both framings are accurate, but they tell a different emotional story, and it’s worth holding onto the smaller, absolute number to keep the finding in proper perspective.
Finally, one related and even more dramatic claim deserves particular caution. A separate study suggesting GLP-1 drugs might reduce the risk of death after a breast cancer diagnosis by 91% prompted visible skepticism even from physicians generally enthusiastic about these medications, with one commentator directly questioning whether a number that large was “too good to be true.” That level of self-correction within the medical community is actually a healthy sign — it suggests the field is treating even exciting findings with real scrutiny rather than running ahead of the evidence.
What This Doesn’t Mean
Given how quickly exciting medical findings can get oversimplified once they leave a research conference and reach the wider internet, a few things are worth stating clearly.
This does not mean GLP-1 drugs are an approved or recommended treatment for breast cancer prevention. They remain approved specifically for type 2 diabetes, weight management, and a small number of other indications, including cardiovascular risk reduction and obstructive sleep apnea. Using them specifically to try to prevent breast cancer, outside of those approved uses and without medical guidance, isn’t supported by current evidence or guidelines.
It also doesn’t mean every woman taking a GLP-1 medication is now meaningfully protected from breast cancer. This is population-level data showing a statistical association across tens of thousands of people, not a guarantee or a precise prediction for any single individual.
And it doesn’t resolve why this is happening. Even the researchers most excited about the finding are explicit that the next required step is a properly designed prospective trial, and that until then, this remains a promising, hypothesis-generating signal rather than an established, causal protective effect.
Read more Scientists Finally Explain Why Some People Eat Less But Still Gain Weight
Why This Finding Still Matters
None of the caveats above make this finding unimportant. Breast cancer screening and treatment improvements have already driven a substantial decline in breast cancer deaths over recent decades, and finding a genuinely new, scalable prevention strategy on top of that would be significant, particularly for a disease where effective prevention options have historically been limited.
The fact that multiple independent research groups, using different cohorts and somewhat different methods, arrived at broadly similar directional findings within the same research cycle adds some weight to the signal, even while each individual study carries the same observational limitations on its own. Dr. Iyengar’s framing captures the appropriately balanced reaction within oncology: describing this as an exciting new frontier that could meaningfully change the field, while being equally clear that randomized clinical trials are still needed to understand how, or whether, these drugs should actually be used for this purpose.
The Bottom Line
Multiple studies presented at ASCO’s 2026 annual meeting found that women taking GLP-1 medications were diagnosed with breast cancer meaningfully less often than women who weren’t, with effect sizes ranging from roughly 16% to 47% depending on the specific study and population. Researchers have proposed plausible biological mechanisms beyond simple weight loss, including reduced insulin resistance and lower inflammation, though weight loss itself likely remains a major contributor.
The honest, current status of this research is “promising and worth pursuing further,” not “proven.” The scientists behind these findings have been unusually direct in saying so themselves, calling for the prospective, causally-informative trials that observational data like this can’t provide on its own. That’s a genuinely exciting place for the research to be — it just isn’t yet a place where the finding should change how anyone thinks about GLP-1 medications outside of their currently approved uses.
Frequently Asked Questions
Does this mean GLP-1 drugs are approved to prevent breast cancer?
No. GLP-1 medications remain approved for type 2 diabetes, weight management, and a small number of other specific conditions. They are not currently approved or recommended as a breast cancer prevention treatment, and the researchers behind these studies have explicitly said more research is needed before any such recommendation could be made.
Is this finding based on a clinical trial?
No, these are observational, retrospective studies that compared existing health records of women who did and didn’t take GLP-1 medications. This type of study can identify a strong statistical association but cannot prove the medication directly caused the lower cancer rates. Researchers are calling for a prospective clinical trial to clarify that.
Is the breast cancer risk reduction just from losing weight?
Likely a significant part of it, but probably not the whole story. Researchers have pointed to additional mechanisms, including reduced insulin resistance and lower inflammation in fat tissue, that may contribute independently of weight loss itself.
How big is the actual risk reduction in real terms?
The relative risk reduction was about 30% in the largest study, but the absolute difference was smaller — roughly seven fewer breast cancer cases per 1,000 women studied. Both numbers are accurate; the relative figure sounds more dramatic, while the absolute figure better reflects the real-world size of the effect.
Should women take GLP-1 medication specifically to lower their breast cancer risk?
This isn’t supported by current evidence or medical guidelines. GLP-1 medications carry their own risks, side effects, and considerations that should be discussed with a doctor based on approved uses, rather than started specifically as a cancer-prevention strategy based on early observational findings.
This article is for informational purposes only and does not constitute medical advice. GLP-1 medications are not currently approved or recommended specifically for cancer prevention. Please consult a healthcare professional regarding appropriate use of these medications and your individual cancer risk factors.